
Hocus Pocus for Aortic Stenosis in the ED
Morgan Uebelacker, MS4, University of Kentucky College of Medicine
Kenneth Dumas MD, PGY-2 University of South Florida – Emergency Medicine
Charlotte Derr, MD, RDMS, FACEP University of South Florida – Emergency Medicine
Background info
In honor of Halloween coming up, lets discuss how a little ~hocus pocus~ can help us identify valvular heart disease, specifically aortic stenosis, in the emergency department. On our board exams, AS is classically seen in an older patient presenting with syncope, angina, and/or dyspnea. On physical exam, they are found to have a harsh, late-peaking systolic murmur at the right upper sternal boarder that radiates to the carotids. Unfortunately, this classic symptom triad isn’t usually present until late in the disease process meaning if we wait for those symptoms, there may already be irreversible damage to the heart. Symptomatic AS patients have a mortality rate of about 25% per year [1]. Given the effectiveness and availability of transcatheter aortic valve replacement (TAVR), early identification of AS is crucial to prevent progression to severe disease and is something that we can do, even in the middle of the busy ED, to decrease morbidity and mortality for these patients.
Much like the Sanderson Sisters did in the beloved Halloween classic, point of care ultrasound (POCUS) has put a spell on us all. Thus, you have probably all heard that cardiac auscultation via stethoscope is falling to the wayside in favor of echocardiography. In fact, many studies have demonstrated that, regardless of level of training or experience, cardiac auscultation is not accurate when it comes to identifying valvular heart disease [2]. Luckily, there is an US machine on nearly every corner in the ED and bedside US can help us identify abnormalities that might help us narrow our differential.
So, let’s demystify this process and walk through a case
A 66-year-old male comes into the ED presenting for shortness of breath and lightheadedness. You walk over to start taking a history and learn that he was outside watering plants and lifts a 20lb jug of water. During this episode of exertion, he felt significantly more short of breath and tachycardic, soon becoming lightheaded.
ROS: (+) Shortness of breath
PE: (+) Systolic harsh, crescendo/decrescendo murmur, (-) rales, wheezes, tachypnea (-) RRR
Social: Negative for ETOH, Tobacco, and Drugs
Labs: (+) Cr 1.4, BUN 22, Troponin (0.021)
After hearing the murmur you grab your handy ultrasound, squeeze out some gel, and place the probe on the patient and then…
You obtain a beautiful parasternal long view
Here you’ll want to examine the echogenicity of the valve and the relative mobility of the leaflets
As you’d expect, a stenotic aortic valve will appear hyper-echoic on ultrasound and may have decreased mobility.
Move onto your parasternal short
and finally, your apical 5-chamber view
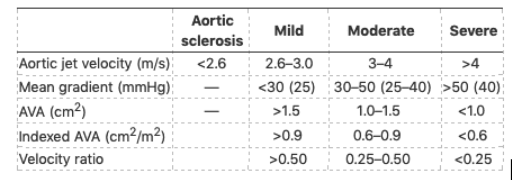
Pro-tip/Pearl: These two-dimensional findings can also be seen in clinically insignificant aortic sclerosis; thus, it is important to differentiate these distinct diagnoses. This is where spectral doppler comes in, allowing us to assess aortic jet velocity and pressure gradients across the valve and more reliably identify clinically significant AS.
Now, if you’re like me and spook easily at the sight of the phrase “jet velocity”, and if the words “pressure gradient” give you a case of the “heebie-jeebies”, you might be wondering if these calculations would be better left in the hands of expert echocardiographers. However, you can rest assured knowing that several studies have demonstrated the reliability of POCUS at identifying AS, even with novice sonologists manning the probe [4-6].
With that in mind lets get down to the real magic of bedside POCUS in AS.
To examine jet velocity, you need to obtain an apical 5-chamber view. Jet velocity is best assessed in an apical-5-chamber view because this places the US beam parallel to the direction of the blood flow out the LV through the aortic valve. Consider using color doppler to help you identify flow through the LVOT.
On the trusty US of your choice, you’ll want to select the continuous wave (look for the CW button) doppler setting. It is important to note that continuous wave doppler is used here because it is better than pulsed wave doppler at visualizing the higher velocities that are seen with a stenotic valve. Continuous wave doppler can be used at the same time as color doppler.
The continuous wave doppler line is then placed through the LVOT with the area of interest being the level of the aortic valve as seen below. Use the beam steering function as needed to make sure the CW doppler line is parallel to the direction of flow out of the LVOT.

Once you obtain this view, push CW again, and you will be able to see the doppler tracing with jet velocities located below the baseline (this represents flow AWAY from the probe). Freeze the image.
Now measure the peak of the jet velocity on the Y-axis of the tracing. Peak velocity can be measured using the tallest curve.

An aortic jet velocity between 3-4 m/s indicates moderate disease while a velocity >4 m/s indicates severe stenosis [7].
While every US can be slightly different here’s a video below showing how to easily set this up on a GE Venue Go.
Pearl: Use caution when using this method in low cardiac output states because the reduced contractility won’t generate a pressure gradient that accurately reflects disease severity. Conversely, concurrent aortic regurgitation may lead to overestimated peak velocities.
Case Wrap-Up
Congratulations, your sharp POCUS skills helped successfully identify potential aortic stenosis. The patient was transferred upstairs where they received a formal echocardiogram and evaluation for valve replacement. The patient successfully underwent TAVR placement and was safely discharged home
ED workup and POCUS evaluation can potentially lead to earlier diagnosis and may avoid the morbidity associated with untreated severe aortic stenosis. If the magic of POCUS in aortic stenosis has captured your focus, then you may enjoy the following post from emDocs as well: http://www.emdocs.net/pocus-for-aortic-stenosis/
References
Strojny J, Taylor L. Did you hear that murmur? No, but I saw it on ultrasound! - A Clinical Case of Aortic Stenosis. ACEP Emergency Ultrasound Section Newsletter. 2021 April; https://www.acep.org/how-we-serve/sections/emergency-ultrasound/news/april-2021/did-you-hear-that-murmur-no-but-i-saw-it-on-ultrasound---a-clinical-case-of-aortic-stenosis/
Otto CM. Heart 2018;104:1807–1808
Lopez M, Dornhecker C, Chambers KA, Gordon Jr. R. POCUS for Aortic Stenosis. emDocs blog post. 2020 May; http://www.emdocs.net/pocus-for-aortic-stenosis/
Gulič TG, Makuc J, Prosen G, Dinevski D. Pocket-sie imaging device as a screening tool for aortic stenosis. Wiener klinische Wochenschrift. 2016 May 1;128(9-10):348-53.
Cowie B, Kluger R. Evaluation of systolic murmurs using transthoracic echocardiography by anaesthetic trainees. Anaesthesia. 2011 Sep;66(9):785-90.
Frederiksen CA, Juhl-Olsen P, Andersen NH, Sloth E. Assessment of cardiac pathology by point-of-care ultrasonography performed by a novice examiner is comparable to the gold standard. Scandinavian journal of trauma, resuscitation and emergency medicine. 2013 Dec;21(1):87.
Vahanian A, Otto CM. Risk stratification of patients with aortic stenosis. Eur Heart J. 2010 Feb;31(4):416-23. PMID: 20047994
https://www.youtube.com/watch?v=RDPaeCqfA2Y 🡪 Point-of-Care Echo: aortic Stenosis vs. Sclerosis
Edited by Michael Weaver, MD