
Airway POCUS: Cricothyrotomy
Lance Lewis, MD and Allyson Hansen, DO
Overview
Cricothyrotomy is a rarely performed procedure by the emergency physician, but can be life- saving and is critical to know. Compound this with physician nerves and a non-ideal airway anatomy secondary to body habitus and trauma, this can be a difficult procedure to perform! Thankfully, ultrasound can be used as an adjunct to properly identify airway anatomy.

Image 1 (1). The cricothyroid membrane can be identified between the thyroid cartilage and the cricoid cartilage, which can be seen in the longitudinal picture below. Thyroid cartilage is a hypo-echoic structure most superior (picture left) connected to the other also hypo echoic cricoid cartilage via a bright, hyper echoic linear air mucosal border of the membrane. This membrane is the cricothyroid membrane (CTM).
(Th – thyroid cartilage; CTM – cricothyroid membrane; Cr – cricoid cartilage)
Multiple case series have described identifying the cricothyroid membrane under ultrasound guidance. A 2018 report describes a patient with a deep neck abscess that was admitted to the hospital for surgical drainage. Unfortunately, the patient developed progressive airway compromise prior to surgery and needed emergent airway control. Due to the swelling secondary to the abscess, the cricothyroid membrane could not be palpated and with the use of ultrasound was actually found to be much more lateral then what was initially predicted (2).
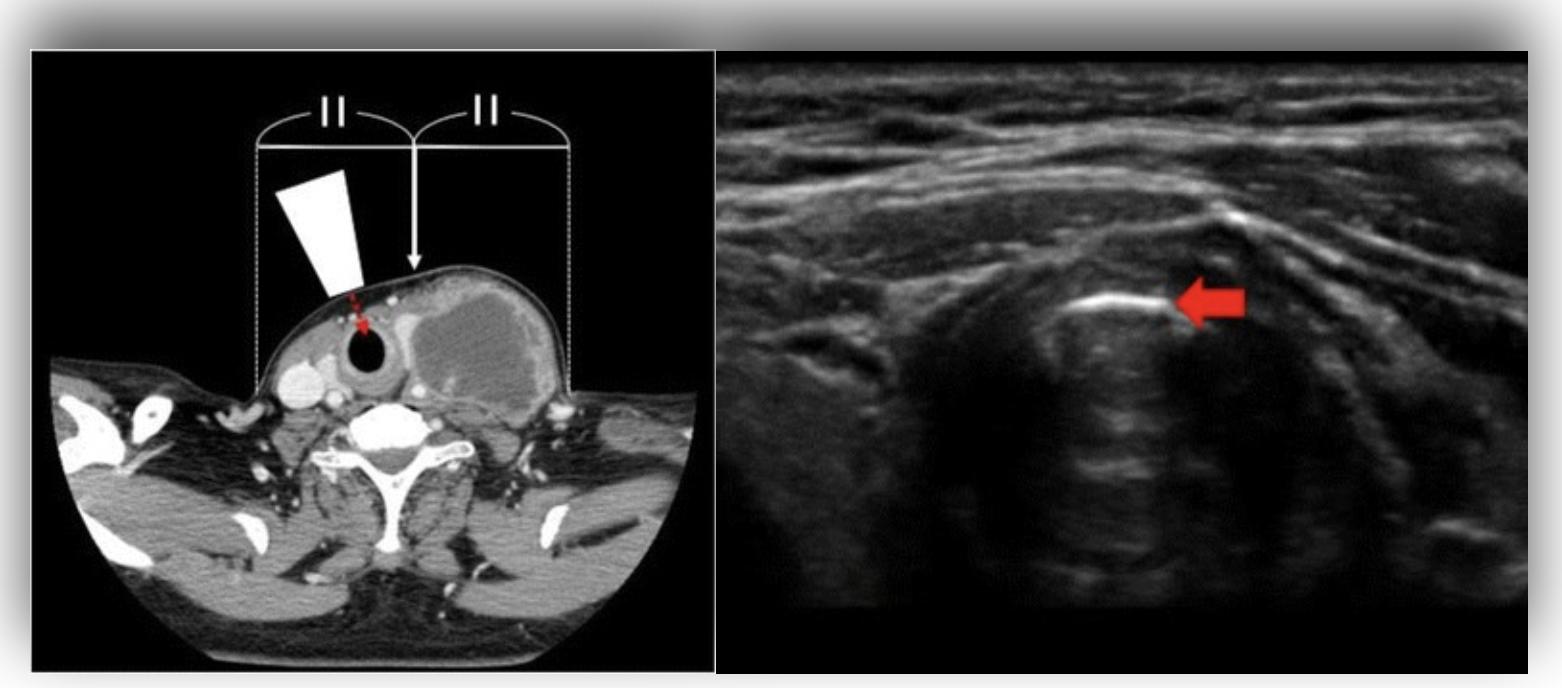
Image 2. A transverse POCUS image of the cricothyroid membrane (RIGHT) is displayed. The hyperechoic membrane with air filled larynx is seen in the far field. Air posterior to a reflective surface creates reverberation artifact or A-lines. This is seen deep to the membrane. The image to the LEFT is a CT showing the laterally displaced cricothyroid membrane.
Interestingly, the American Society of Anesthesiologists also has an article on using ultrasound to identify the cricothyroid membrane for tracheal anesthesia in the setting of awake, fiberoptic guided intubation (3). In this case, a needle attached to a syringe containing lidocaine is passed through the cricothyroid membrane under direct visualization with the ultrasound while applying negative pressure to the syringe. Once air is aspirated, the lidocaine can be applied to the trachea. While this may not necessarily be something that would be used frequently by us emergency physicians, it would be an interesting tool to have at our disposal for some of those trickier awake intubations.
In 2012 a new novel technique of ultrasound guided, bougie assisted cricothyrotomy was described (4). During this study, operators would view the cartilaginous structures with the linear probe in the long axis and the cricothyroid membrane was cut under ultrasound guidance with a scalpel. A bougie was then inserted and an endotracheal tube was passed over this similar to the “scalpel, finger, bougie” technique that we are all educated on. Interestingly, this study showed a 95% success rate (1). Recall that crichothyroidotomy can be performed in adults. We generally do not perform this procedure in children age <8 (see more information about transtracheal jet insufflation or needle crichothyroidotomy).
How to Perform Ultrasound Assisted Crichothyroidotomy
1. Patient in flat position
2. Stand at side of patient (depending on your dexterity)
3. Using linear probe, identify cricothyroid membrane in both a sagittal and transverse plane (4). Define Anatomy and landmarks on screen
5. Mark your spot with sterile marking pen
6. Prepare and drape pa'ent in sterile fashion
7. Make generous vertical incision through skin overlying the cricothyroid membrane
8. Make horizontal incision through cricothyroid membrane
9. Insert pinky finger on non-dominant hand into newly created stoma
10.Using dominant hand, insert introducing bougie into stoma
11.Pass 6.5 endotracheal tube over bougie
12.Remove bougie and either use bag valve ventilation or connect to mechanical ventilator
Summary
In summary, cricothyrotomy is a rarely performed, but a critical lifesaving procedure that the emergency physician can perform. Under certain circumstances, palpation of anatomy may not be feasible. Also, utilizing POCUS for a perceived difficulty airway and marking your membrane beforehand can be a way to cognitively offload and feel more confident taking over someone’s airway. Start practicing finding the airway anatomy on your healthy patients with ultrasound so when the time comes, and it will, you’ll be ready!
For more information and instructional videos, check out:
How to POCUS the anterior neck for airway anatomy.
How to perform a crichothyrotomy with Bougie.
Citations
Identification of the Cricothyroid Membrane (CTM). Pocus Can Be Used to ...https:// www.researchgate.net/figure/Identification-of-the-cricothyroid-membrane-CTM-POCUS- can-be-used-to-identify-the-CTM_fig3_357975449.
Okano, Hiromu, et al. “Ultrasound-Guided Identification of the Cricothyroid Membrane in a Patient with a Difficult Airway: A Case Report.” BMC Emergency Medicine, vol. 18, no. 1, 2018, https://doi.org/10.1186/s12873-018-0156-7.
Suzuki, Akihiro, et al. “Ultrasound-Guided Cannula Cricothyroidotomy.” Anesthesiology, vol. 117, no. 5, 2012, pp. 1128–1128., https://doi.org/10.1097/aln.0b013e3182531a6c.
Lawer, T., and J. Lin. “403 Feasibility of Training for Ultrasound-Guided Cricothyrotomy Using a Novel 3-D Printed Training Model Simulating a Difficult Cricothyrotomy with Thick Pre-Tracheal Neck Tissue.” Annals of Emergency Medicine, vol. 80, no. 4, 2022, https:// doi.org/10.1016/j.annemergmed.2022.08.421.
